
Workforce, Workload, and Burnout in Critical Care Organizations: Survey Results and Research Agenda
 Lilly, Craig M. MD, FACP, FCCP, FCCM1; Oropello, John M. MD, FACP, FCCP, FCCM2; Pastores, Stephen M. MD MACP, FCCP, FCCM3; Coopersmith, Craig M. MD, FACS, FCCM4; Khan, Roozehra A. DO, FCCP5; Sessler, Curtis N. MD, FCCP, FCCM6; Christman, John W. MD7; for the Academic Leaders in Critical Care Medicine Task Force of the Society of Critical Care Medicine Author Information
Lilly, Craig M. MD, FACP, FCCP, FCCM1; Oropello, John M. MD, FACP, FCCP, FCCM2; Pastores, Stephen M. MD MACP, FCCP, FCCM3; Coopersmith, Craig M. MD, FACS, FCCM4; Khan, Roozehra A. DO, FCCP5; Sessler, Curtis N. MD, FCCP, FCCM6; Christman, John W. MD7; for the Academic Leaders in Critical Care Medicine Task Force of the Society of Critical Care Medicine Author Information 
1Department of Medicine, University of Massachusetts Medical School, Worcester, MA.
2Department of Surgery, Mount Sinai Medical Center, New York, NY.
3Department of Anesthesiology and Critical Care, Memorial Sloan Kettering Cancer Center, New York, NY.
4Department of Surgery, Emory Critical Care Center, Atlanta, GA.
5Department of Surgery, University of Southern California, Los Angeles, CA.
6Department of Internal Medicine, Virginia Commonwealth University, Richmond, VA.
7Department of Internal Medicine, The Ohio State University Wexner Medical Center, Columbus, OH.
*See also p. 1692.
All the authors report that they are leaders of Critical Care Organizations.
Dr. Lilly received support for article research from the National Institutes of Health. Dr. Pastores received funding from McGraw Hill Publishers (royalties) and Cleveland Clinic (Grand Rounds speaker). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Address requests for reprints to: Craig M. Lilly, MD, Professor of Medicine, Anesthesiology, and Surgery, University of Massachusetts Medical School, UMass Memorial Medical Center, 281 Lincoln Street, Worcester, MA. E-mail: craig.lilly@umassmed.edu
Critical Care Medicine: November 2020 – Volume 48 – Issue 11 – p 1565-1571
doi: 10.1097/CCM.0000000000004552
Abstract
This report provides analyses and perspective of a survey of critical care workforce, workload, and burnout among the intensivists and advanced practice providers of established U.S. and Canadian critical care organizations and provides a research agenda.
A 97-item electronic survey questionnaire was distributed to the leaders of 27 qualifying organizations.
United States and Canada.
Leaders of critical care organizations in the United States and Canada.
None.
We received 23 responses (85%). The critical care organization survey recorded substantial variability of most organizational aspects that were not restricted by the critical care organization definition or regulatory mandates. The most common physician staffing model was a combination of full-time and part-time intensivists. Approximately 80% of critical care organizations had dedicated advanced practice providers that staffed some or all their ICUs. Full-time intensivists worked a median of 168 days (range 42–192 d) in the ICU (168 shifts = 24 7-d wk). The median shift duration was 12 hours (range, 7–14 hr), and the median number of consecutive shifts allowed was 7 hours (range 7–14 hr). More than half of critical care organizations reported having burnout prevention programs targeted to ICU physicians, advanced practice providers, and nurses.
The variability of current approaches suggests that systematic comparative analyses could identify best organizational practices. The research agenda for the study of critical care organizations should include studies that provide insights regarding the effects of the integrative structure of critical care organizations on outcomes at the levels of our patients, our workforce, our work practices, and sustainability.
The Society of Critical Care Medicine (SCCM) convened a taskforce of Academic Leaders in Critical Care Medicine (ALCCM) to develop a series of consensus articles with toolkits for advancing critical care organizations (CCOs) (1–3). We defined CCOs as organizations that have an advanced governance structure headed by an intensivist physician that has primary governance over the majority, if not all, of the ICUs and critical care operations of the healthcare organization or medical center (4). CCOs serve healthcare organizations by providing physician-led primary governance for most of the organization’s ICUs. The articles of this series have defined the vertical (relation to institutional leaders) and horizontal (interdepartmental) integration of critical care delivery for healthcare organizations and the methods by which CCOs promote patient safety, high quality care, research, education, and professional development. A third article presented a narrative review of the issues related to the critical care workforce, workload, and burnout syndrome (BOS) among intensivists and advanced practice providers (APPs) and identified that the lack of published data about CCOs limits our ability to design a CCO research agenda (3). The ALCCM group designed and SCCM supported the development of a 97-item survey to gather foundational facts about CCOs from the leaders of 27 functioning CCOs. The items of the survey provide information about CCO structure, workforce, work environment, and records the diversity of their intensivists. The main aim of the presentation of its analyses and results is to encourage research that fills emerging gaps on our knowledge of CCO structure by defining a research agenda.
METHODS
The leaders of CCOs were contacted after identification from web searches for content containing the terms “Critical Care or Intensive Care Department, Center, System, Institute, Operations Committee, Service or Product Line or Hospital” performed in April 2014. These CCO leaders provided contact information for other centers that might have also met the prespecified CCO definition, in all 37 potential CCOs provided descriptions of their structure. Twenty-seven healthcare organizations, 23 in the United States and four Canadian met the prespecified CCO definition above. A 97-item survey instrument was developed for delivery on the Survey Monkey platform that captured structural, workforce, and burnout domain information using the processes presented in Figure 1. After validation by previously described methods including comparison to objectively measured workplace metrics and pilot testing (5), the survey was deployed. The leaders of the institutions with CCOs presented in “italic” font in Table 1 were invited on behalf of the ALCCM by John W. Christman, MD; J Christopher Farmer, MD, FCCM; Craig Coopersmith, MD, FCCM; Jose L. Diaz-Gomez, MD, FCCM; Stephen M. Pastores, MD, FCCM; and Vladimir Kvetan, MD, FCCM, to participate in the survey without compensation. Strength of association was measured by cubic regression.

bThe Cleveland Clinic has two CCOs.
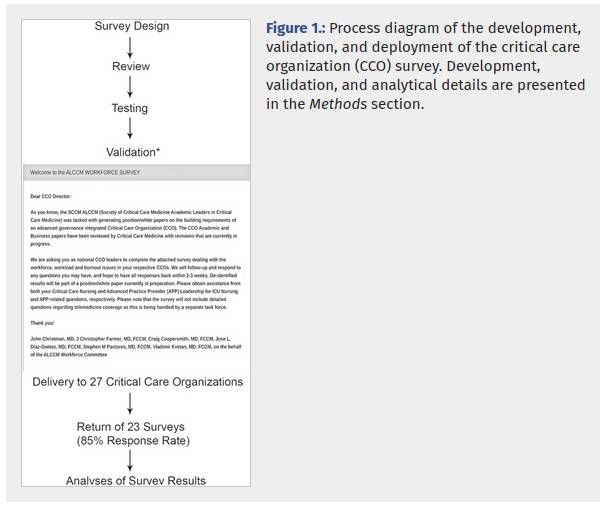
Monthly e-mail reminders were sent to nonresponders who were also contacted by phone to confirm that they had received the invitation. The structure of the survey platform allowed only one consensus response from each CCO and reported only site-deidentified data. In all, 23 of the 27 institutions (85%) initially invited on July 12, 2017 completed the survey by May 30, 2019. The 97-item survey is provided as an electronic supplement. The survey was conceived, created, and refined by the SCCM ALCCM Task Force in the context of its charge to provide current and actionable information on the state of the critical care workforce to the SCCM. Survey data informed SCCM leaders and task force members with research expertise in support of an iterative process to develop an expert opinion-based research agenda.
Survey Results
The overall response rate was 85% (23/27). Results stratified by survey domain are presented for 80 of the 97 survey items. Items were not included when the information was nearly identical to that presented for a similar item. For example, the exclusion of the response pattern for part-time physicians was not included because it was nearly identical to that of full-time physicians. Items with nonmeaningful numbers of responses, for example, starting salaries, and free text only items were excluded.
CCO Characteristics
The adoption of the CCO model does not appear to be restricted to institutions of large size as some institutions with as few as two ICUs at their main institution have implemented a CCO. CCO leaders reported that the number of ICU, stepdown or progressive care beds at the main institution covered by their CCOs ranged from 18 to 400 (mean 123.5; median 95; interquartile range [IQR] 60–139). The number of CCO covered beds at affiliated hospitals ranged from 0 to 235 (mean 57; median 95; IQR 0–100). CCOs reported that 68% of the beds that they administered were located at their main institution.
Most leaders reported that their CCOs support a variety of specialty dedicated ICUs with only a single CCO using a uniform ICU type model (mixed ICU, e.g., medical-surgical). The median number of different specialty unit types (not counting mixed ICUs) that CCOs governed was 4 (mean 4.5; range 0–9; IQR 3–6). The rank order frequency of reported ICU bed types were medical, other (unspecified), surgical, cardiothoracic, neurosciences, cardiac, pediatric, transplant, trauma, and burn beds.
The majority of senior leadership positions for the institutions that have adopted CCOs are held by physicians. The CEO is a physician for 11 and a nonphysician for eight CCOs of the 19 CCOs that responded to this item. The College of Medicine Dean is a physician for all 17 reporting institutions, the President is a physician for 12 and is a nonphysician for seven of 19 responding institutions, and the Chief Medical Officer is a physician for 21 and a nonphysician for a single institution. In addition to a CCO leader, 17 of 22 reporting CCOs had directors for department-based critical care service lines. All 23 CCOs reported that they have a dedicated Medical Director for each of their medical center ICUs, 11 CCOs report also supporting Associate ICU Directors, and one CCO reported that some of their rural hospital ICUs did not have a dedicated medical director. All 23 CCOs reported participating in regularly scheduled intraorganizational and interdepartmental meetings.
Regularly scheduled staff surveys were used to solicit provider input by 22 of 23 CCOs. Periodic retreats that provided a forum for interactive discussion and teambuilding were used by 11 of 23 CCOs. The atmosphere or culture of critical care was rated by CCO leaders as an 82 ± 12 mean and sd with a range of 59–100 on a 0–100 (more positive) scale.
CCO Physicians and Clinical Staff
Workforce characteristics of the physicians and clinical staff of the CCOs are presented in Table 2.
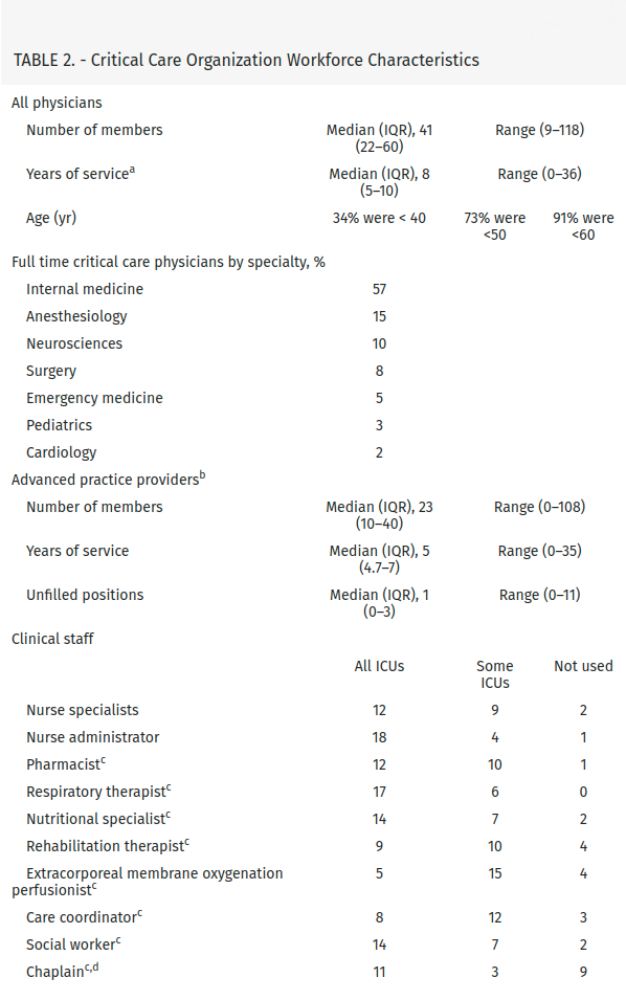
aThe years of service was not meaningfully different for programs that offered service duration-based accommodations and those that did not.
bOne critical care organization reported that it did not use ICU advanced practice providers.
cThe survey item used the term dedicated.
dReligion based support staff.
Physicians
The survey asked the leaders of CCOs to share their institutions definition of a of a full-time critical care physician. Forty-four percent of the respondents indicated that full time at their institution was defined as more than 50%, 30% defined it as more than 80%, and 30% defined it as 100% effort spent in CCO related clinical, education, research, or administrative activities. There is also substantial variation of the number of physicians that CCOs employ. Group size ranged from nine to 118 physicians that their institution classified as full or part time with a median of 41 and an IQR of 22–60. The majority of physicians were classified as full time with part-time physicians ranging from 0 to 38 individuals and per diem physicians ranging from 0 to 7 individuals.
Advanced Practice Providers
The APPs of 21 programs reported working on weekends, and 18 indicated that their APPs worked overnight. Graduated experience-based and revenue-based compensation models for APPs were reported by three each of the 21 CCOs. The APPs of four CCOs could be awarded an academic rank. The reported range of annual vacation time was 4–6 weeks. Professional training was offered by 17 of 18 responding CCOs, and 18 provided funding for medical education. An APP Training program was supported by 10 of the 21 CCOs.
Critical Care Workload
The majority of CCOs assign their intensivists responsibilities that are not related to direct care of their ICU patients at the same time that they are signed in as responsible for the patients of their ICUs. These additional activities include performing consultations, leading cardiac arrest or rapid response teams, performing operative procedures, performing bedside procedures, providing ICU telemedicine evaluation and management services, providing outpatient services, or managing stepdown unit patients. The physicians of 14 CCOs have responsibilities outside of their ICUs, and the intensivists of nine CCOs provide services only in their ICUs during weekdays. Many CCOs expand coverage responsibility off-hours with only five CCO’s intensivists providing only ICU services during weeknights, three during weekend days, and two during weekend nights. A shortage of ICU physicians was reported by six of 23 responding CCOs. The range of unfilled intensivist positions was 2–3 with no CCOs reporting single vacancies. The average 5-year attending intensivist attrition rate was 9.5 ± 6 (sd) %.
The number of ICU beds covered by the CCO to the number of attending physician FTE ratios ranged from 0.7 to 10 with a median of 2.5 (IQR 1.7–4) and a mean of 3.1 ± 2 (sd). The number of patients a CCO attending physician covers during a weekday ranged from 8 to 30 with a median of 13.5 (IQR 11.5–16.5) and a mean of 15 ± 5 (sd) patients. Patient to physician ratios are higher after hours and on weekends. Attending physicians of all CCOs were supported by residents, fellows, and APPs; however, two CCOs reported that attending physicians worked alone in some of their ICUs. The attending physicians of all CCOs were available at night either using an in-house call system for some (10 CCOs) or all (7 CCOs) ICUs, or a model in which off-duty staffs are called in to the hospital on demand (6 CCOs all ICUs; 10 CCOs some ICUs).
The number of annual shifts worked by a full-time clinical faculty member ranged from 42 to 192 with a mean of 156 ± 43 (SD) and a median of 168 with an IQR of 143–186 (168 shifts corresponds to 24 7-d wk). Shift duration was reported to range from 9 to 14 hours, with a median of 12 with an IQR of 10–12 and a mean of 11 ± 1.5 (SD) hours. All CCOs limited the number of consecutive shifts that could be worked without a 24 hour no service interval. The range of consecutive shifts allowed was 1–14, with a median of 7 with an IQR of 5–7 and a mean of 6 ± 1.2 (sd) days. The number of consecutive night shifts allowed was lower with only two CCOs allowing more than six consecutive night shifts. The annual number of weekends worked by attending physicians ranged from 6 to 20 with a median of 12 with an IQR of 10–15 and a mean of 13 ± 3.3 (sd) days. The range of protected time offered by 13 responding CCOs was 0–50% with a mean and median of 20%. Vacation time per years of service (queried in 5 yr increments from 0 to 29 and > 30) ranged from 3 to 7 weeks with a median of 4.5 and an IQR of 4–5 for faculty with less than 15 years of service and ranged from 3.5 to 7.5 weeks with a median of 5.5 and an IQR of 4–6 weeks for those with more than 15 years of service.
CCO leaders rated the work life balance of their critical care physicians at a 64 ± 24 (sd) on a scale of 0–100 (higher indicates better balance) with a range of 15–99.
The leaders of all CCOs reported high default nurse to patient ratios with 14 CCOs reporting 1:2 ratios, two reporting 1:1 ratios, and two reporting 1:1 or 1:2 ratios for their ICUs. CCOs that were able to provide 1:1 ratios listed complex device management (continuous veno-venous hemodialysis, extracorporeal membrane oxygenation, intra-aortic balloon pump, left ventricular assist device), postcardiac surgery ICU arrival, severe burn care, and physiologic instability as the indications. The range of the number of available ICU nurse positions was 1–70 among the six CCOs that reported unfilled job postings (6).
Burnout and Well-Being
Programs to address burnout and promote well-being are available at 19 of the 23 reporting CCOs. The hospital is the sole program sponsor for 14 programs, CCOs and hospitals both provide programs at four sites, the medical school and practice plan provide the program at one site, and support is not provided at four sites. The burnout prevention programs of 14–18 responding institutions were targeted to ICU physicians, APPs, and nurses, the programs of two institutions focused on physicians and nurses, and two programs were physician supporting. Respondents identified 15 of the 19 programs as being resilience based (7).
The difference between the average do not resuscitate (DNR) rate at ICU admission of 10% and the DNR rate of 75% at time of death in the ICU suggests that a substantial portion of the end-of-life care and support is provided by CCO providers. All CCOs reported that palliative care consultation services were available.
DISCUSSION
The survey results provide an objective cross-sectional view of the CCO workforce, its members, their workplaces, and workload. One theme of the survey results is the diversity and variability of most variables that are not restricted by the CCO inclusion criteria or regulatory mandates (1). The extent of the variation of operational methods suggests that few aspects of organizational approach (e.g., granular aspects of business, clinical, education, and research structures) are so effective that they have been universally adopted. We believe that the lack of established methods and resources to collect, protect, and share reliable information about CCOs has impeded our ability to provide evidence-based guidance regarding optimal CCO organizational characteristics. The development of the CCO survey instrument and information from its initial deployment forms the foundational element of a CCO knowledge base, that with development, can be used to inform operational decisions and identify research opportunities.
Another prominent theme of the survey findings is that the workload of the intensivists of most CCOs is near the sustainable capacity of many of their attending physicians (3,8–13). The survey reported that most attending physicians managed workload with the help of other providers rather than by working as a lone physician (14). The finding that nearly all CCOs placed limits on the number consecutive shifts that physicians could work, without a 24-hour break, appeared to acknowledge that their workloads are not sustainable. Nonsustainable workload is also suggested by the substantial gap between the number of shifts worked and available nonvacation shifts and the number of CCOs that provided protected, educational, or administrative time. Survey items that document the ages of practicing intensivists are skewed to younger physicians and to shorter durations of service suggest that they may be leaving the ICU workforce due to BOS. Recent reports suggest that healthcare systems are modifying workload to improve retention (15). Concern that excessive workload increased risk for BOS (10) is implied by the number of institutions that offered programs to improve well-being including resilience (7,16,17) and teamwork and team dynamics–based (18) counter measures and the fact that some CCOs provided their own BOS programs.
The survey methodology used in this report has important limitations. Key limitations include not including leaders of institutions that do not use the CCO governance as a comparator group and not capturing outcome or patient level data. The instrument was not designed to provide insights into the reasons that institutions elected to form CCOs or about their value proposition relative to alternative organizational schemas.
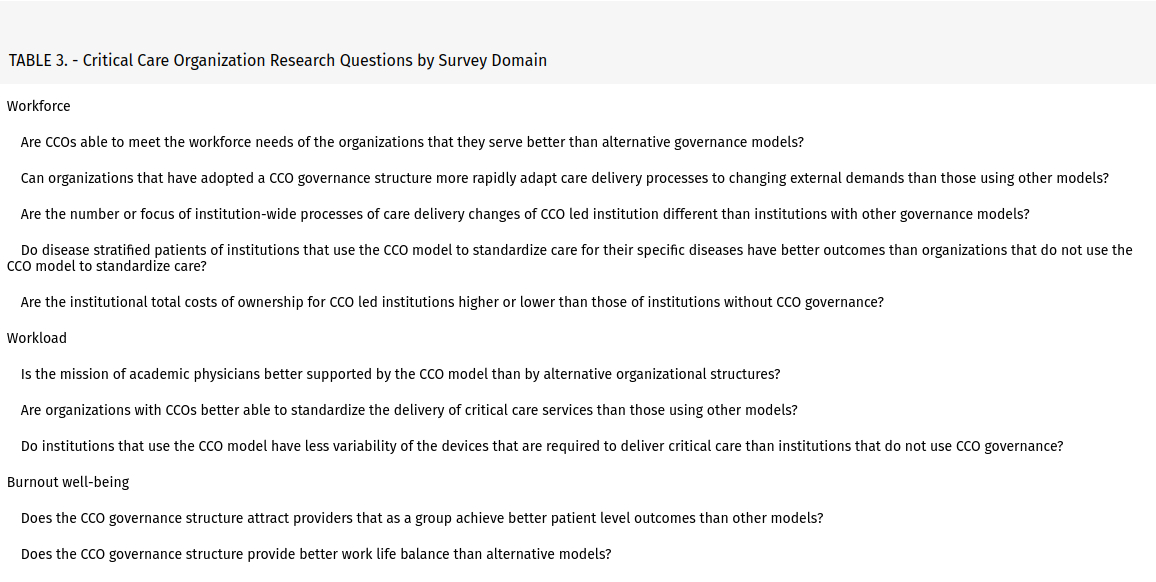
The size, extent, and effort required to establish the U.S. and Canadian CCOs of this report suggest that their importance is sufficient to merit a research agenda (1). The institutional leaders that created these structures that cross traditional organizational boundaries did so with the belief that the financial, service delivery, workforce retention, or patient safety benefits would justify the resources they invested. The research questions, presented in Table 3, allowed current SCCM leaders and experts from the ALCCM Taskforce to define patient, workforce, workflow, and outcome agenda topics that were suggested after analysis of the survey responses from concurrent CCO leaders. The aim of the task force was to provide a nonexhaustive list of consensus topical areas of current interest for active study. The consensus topical areas presented by survey domain in Table 3 should not discourage research into new, evolving, or other important issues that face our growing numbers of CCOs.
Advancing this research agenda will require the collection, protection, and sharing of information across CCOs (19) and with institutions that use other critical care governance models. The creation of the ALCCM group by the SCCM, its generous support of the development of a validated survey instrument, and its deployment represent important advances toward an evidence-based understanding of critical care governance.
Copyright © 2020 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Source: Critical Care Medicine
